
Vitamin B12 - Beyond Deficiency
Like many supplements, B12 has grown in popularity over the past decade and continues to do so as we learn more about its important role in overall health.
VITAMINS
Antonia Mantakaki Wright BSc, MSc
5/29/20264 min read


I am often asked why I am so “obsessed” with Vitamin B12. “Have you checked you B12 levels recently?”, is one of the questions I often ask my clients, friends, family, or people I just met! It is my personal experiences that created that “obsession” but that is a story for another blog. Today I am writing about all the amazing things I have learned over the past few years about B12 through personal research.
Vitamins B12 has traditionally been viewed through a narrow lens: prevent anemia, correct deficiency, and assessment, follow up or root cause analysis stops there. But the conversation around B12 is much broader. Increasingly, clinicians are asking a different question: What level of B12 supports optimal neurological, metabolic, and cognitive function?
This distinction matters because many patients experience fatigue, brain fog, neuropathy, mood changes, and poor stress resilience despite being told their B12 levels are “normal.”
Why “Normal” May Not Be Optimal
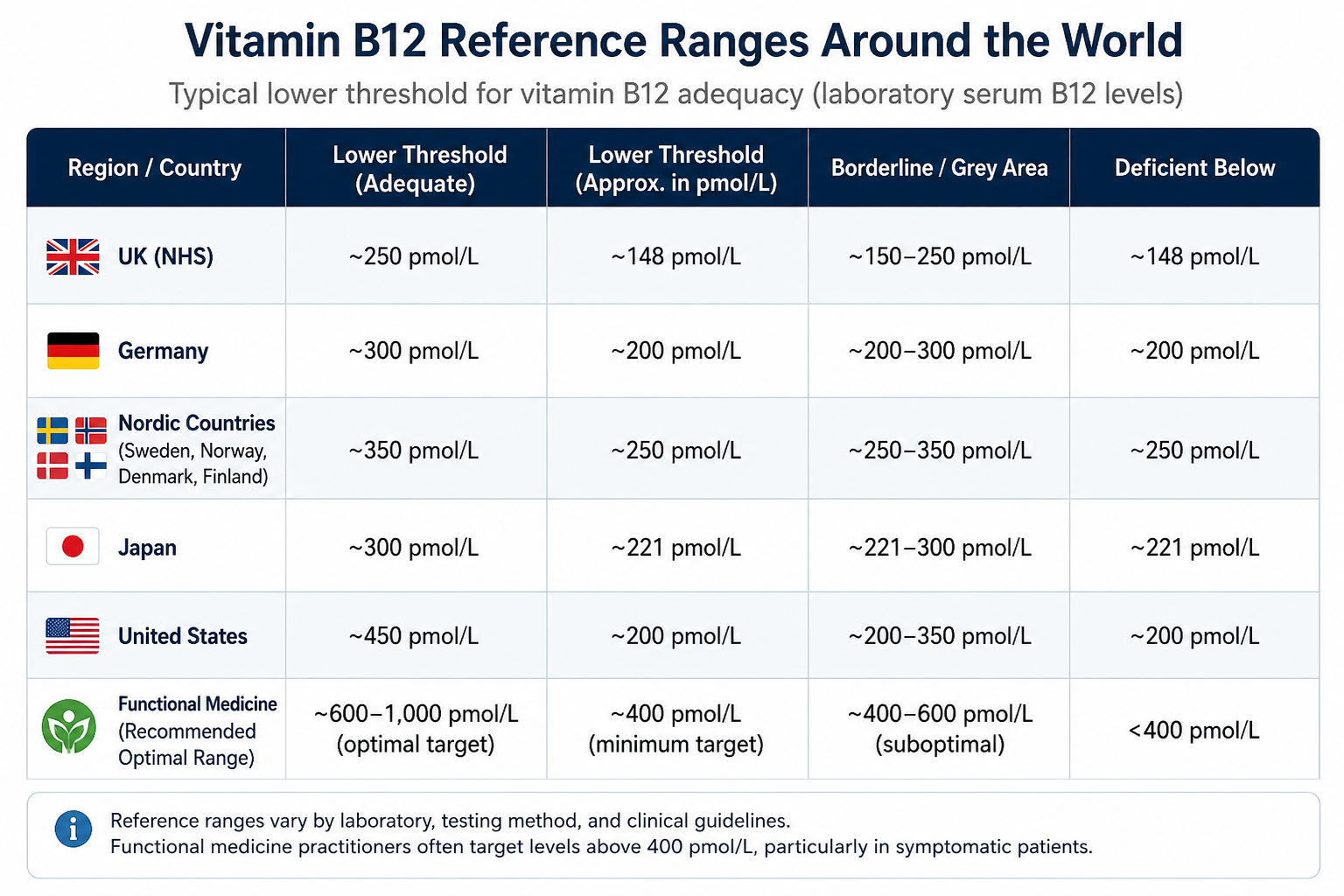
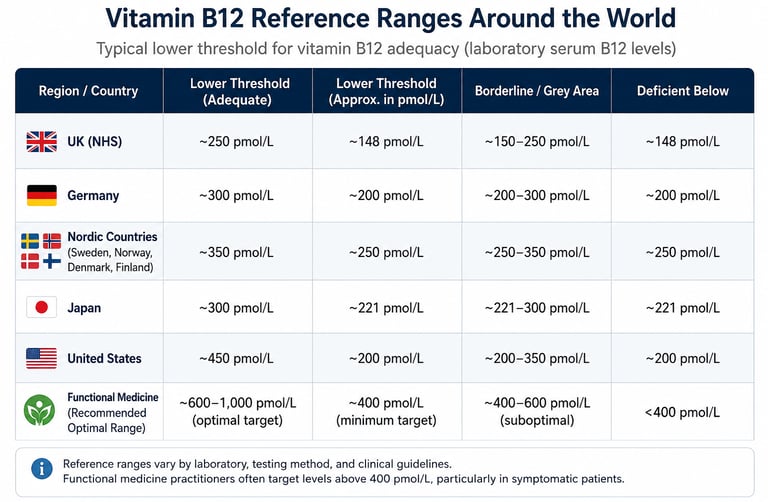
In the UK, conventional laboratory reference ranges often define deficiency below approximately 150pg/mL. However, neurological and psychiatric symptoms may appear well before levels fall this low. Several reviews and clinical discussions note that “low-normal” ranges between 200–400 pg/mL can still be associated with functional deficiency and neurological symptoms. (MSD Manuals)
B12 Matters Beyond Anaemia
Vitamin B12 is essential for:
DNA synthesis
Methylation pathways
Nerve insulation (myelin production)
Neurotransmitter synthesis
Energy metabolism
Homocysteine regulation
When B12 is insufficient at a cellular level, symptoms may include:
Brain fog
Fatigue
Poor concentration
Memory issues
Anxiety or low mood
Tingling or numbness
Dizziness
Sleep disturbances
Reduced stress tolerance
Neurological symptoms can occur independently of anaemia. (MedCase)
Reference ranges vary by laboratory, testing method
This article is for informational purposes only and does not constitute medical advice. Any decisions regarding supplementation, testing, or hormone therapy should be made in consultation with a qualified clinician.
The Gut–B12 Connection: Why Gastrointestinal Health Matters
One of the most overlooked causes of low or suboptimal B12 status is impaired absorption.
B12 absorption is remarkably complex and depends on the correct environmental conditions in the gastrointestinal (GI) track like adequate stomach acid, healthy pancreatic enzymes, proper small intestine function.
This means patients with gastrointestinal conditions are particularly vulnerable to deficiency or poor utilization, including those with:
IBS
Crohn’s disease
Celiac disease
Gastritis
SIBO
History of gastric surgery
Long-term proton pump inhibitor (PPI) use
Metformin use (NCBI)
In these cases, oral supplementation may not adequately raise tissue levels.
Injectable B12 vs Oral Supplements: What’s the Difference?
Oral B12 Supplements
Oral B12 works well for many people, especially when digestion and absorption are intact. However, oral supplements still rely on gastrointestinal uptake. Even high-dose oral B12 can be poorly utilised in people with conditions named above.
Intramuscular administration of B12
Intramuscular administration of B12 (or B12 shots as are now know due to Marketing Agency regulations) bypasses the digestive tract entirely and delivers B12 directly into circulation.
This delivery method potential advantages include faster symptom improvement, better absorption in GI disorders, higher tissue saturation, more predictable delivery and rapid neurological support
Those who have been treated with intramuscular administration of B12 report improvements in, energy levels, mental clarity, mood and stress management, physical stamina and neuropathy symptoms (“pins and needles” on the hand and feet, balance issues, muscle waste, diminished reflexes) sometimes within hours or days after administration, particularly when deficiency or functional insufficiency is significant. That said, responses vary significantly between individuals.
The Misconception: “You Can’t Overdose on B12”
One of the most common myths is that B12 is completely harmless because it is water-soluble. While B12 generally has a strong safety profile, this does not mean unlimited use is risk-free. Potential concerns with excessive or unsupervised use include rosacea flares, sleep disruption, anxiety or overstimulation , imbalances with folate or other B vitamins, masking underlying disease processes. Very high serum B12 without supplementation can also occasionally indicate liver disease, inflammatory conditions, or hematologic disorders. (Nutri Tailor)
The Bottom Line
B12 is not just about correcting severe deficiency or anaemia. For many people, especially those with GI dysfunction, neurological symptoms, fatigue, brain fog, or methylation concerns, can be a meaningful tool. If we look at the functional medicine perspective, optimal health is rarely about chasing the highest number on a lab report. It is about restoring function, improving quality of life, and understanding what the body actually needs to operate well.
Why the Type of B12 Matters
Not all B12 injections are the same and this applies for oral and IM shot. What you should know when buying/booking B12 is: which form is being used, the dose, the frequency.
Common B12 forms include:
Cyanocobalamin
Synthetic form
Most commonly used in conventional medicine
Requires conversion into active forms
Methylcobalamin
Active methylated form
Often favoured in functional medicine
Associated with neurological and methylation support
Hydroxocobalamin
Longer-lasting
Common in Europe
Often used in deficiency treatment
The only recognised body that examines beyond the “normal” ranges is Functional medicine. It is common practice for practitioners to aim for serum B12 levels above 400–500 pg/mL, particularly in symptomatic patients or those with gastrointestinal issues, methylation problems, chronic fatigue, or cognitive complaints. (MyHealthcare). In case you were also wondering why we always encourage clients to seek help from Functional Medicine doctors in addition to their GP.
This approach is based on the understanding that serum B12 does not always reflect intracellular activity, neurological dysfunction can occur before anaemia develops, functional markers such as methylmalonic acid (MMA) and homocysteine may reveal deficiency even when serum B12 appears “normal” (MSD Manuals).
References
O’Leary F, Samman S. Vitamin B12 in health and disease. Nutrients. 2010.
Lachner C, Steinle NI, Regenold WT. The neuropsychiatry of vitamin B12 deficiency in elderly patients. J Neuropsychiatry Clin Neurosci. 2012.
Moore E et al. Cognitive impairment and vitamin B12: a review. Int Psychogeriatr. 2012.
Scalabrino G. Vitamin-regulated cytokines and growth factors in the CNS and elsewhere. J Neurochem. 2009.
Smith AD, Refsum H. Homocysteine, B vitamins, and cognitive impairment. Annu Rev Nutr. 2016.
Hunt A, Harrington D, Robinson S. Vitamin B12 deficiency. BMJ. 2014.
Stabler SP. Vitamin B12 deficiency. N Engl J Med. 2013.
Herrmann W, Obeid R. Causes and early diagnosis of vitamin B12 deficiency. Dtsch Arztebl Int. 2008.
Reynolds E. Vitamin B12, folic acid, and the nervous system. Lancet Neurol. 2006.
Kennedy DO. B Vitamins and the Brain: Mechanisms, Dose and Efficacy. Nutrients. 2016.
11. Amirhossein Mesgarankarimi, A long-standing undiagnosed case of vitamin B12 deficiency: a case report, J Med Case Rep , 2025
Olympian Wellness Ltd trading as Olympian Wellness Clinic
Registered address: 57 High St, Hanham, Bristol, BS15 3DQ
company number: 16675182
© 2026. All rights reserved.


Based and operate at
The Wellness Collective Bristol
57 High Street, Hanham, BS15 3DQ